At ImageWorks, we’ve been helping dental practices make the most of their dental imaging for decades. When it comes to dental cone beam systems, technology has come quite a way since we introduced our first generation 3D dental cone beam system in 2005 when we were called Dent-x.
As technology advances, we are always excited to introduce a dental professional to the power and value of 3D imaging, because it is compelling for so many offices. However, at the same time, with today’s 3D cone beam systems, we also like to say: with great power comes great responsibility. Because of this responsibility, we think it’s important to offer information that allows new users to enter the world of 3D with eyes wide open.
With this goal in mind, we thought it would be worthwhile to provide an overview of some of the most common questions that get asked when dental professionals are looking to implement a Cone Beam system in their office. We hope you find this useful.
What does CBCT stand for?
Sometimes we find it useful to share a quick definition of terms, as different words can be thrown around that have similar meaning. The abbreviation “CBCT” stands for Cone Beam Computed Tomography. Computed Tomography is the general category of 3D medical imaging modalities that includes MRI and CAT Scan systems. The “Cone Beam” refers to the class of CTs that are most commonly used for dental applications. The description comes from the shape of the x-ray beam. Sometimes these systems are referred to as “Cone Beams” or “Dental CTs” or simply Dental 3D imaging systems.
Why is a Cone Beam scan so critical for implant planning?
A dental cone beam can assist dental professionals in many ways. These include:
- Endodontic evaluation
- Impacted teeth related to orthodontics
- Paranasal sinus evaluation
- TMJ visualization
- Trauma evaluation
- Immediate advanced imaging and treatment
However, one of the most common reasons that many dental professionals bring a dental cone beam into their practice is to place implants.
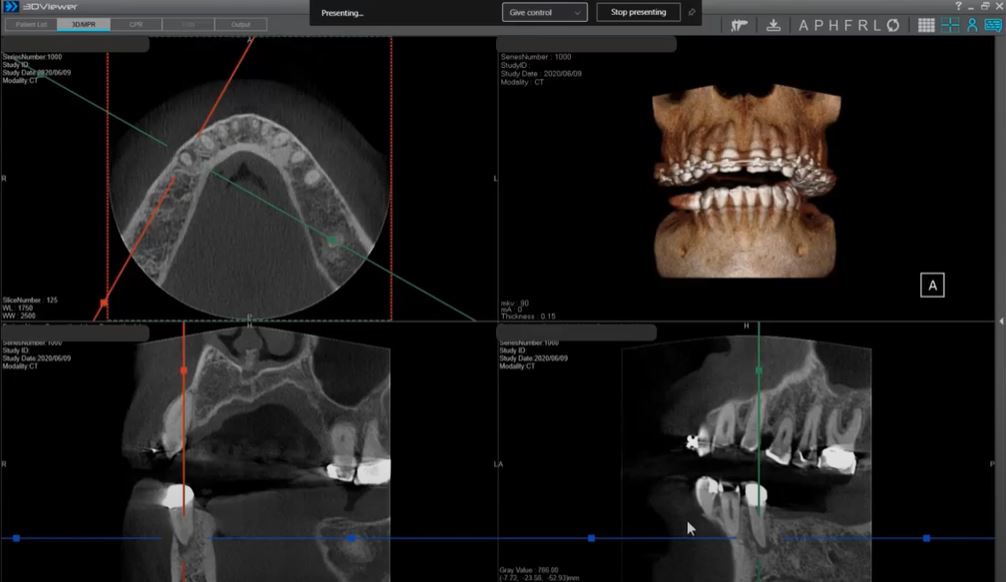
Given this fact, we are going to focus our discussion on this very common application. There are a host of different ways that a Cone Beam system can assist with implant planning. However, one of the most fundamental is providing visibility into the cross-sectional view of the location of the implant. In 2012, the AAOMR published a position paper recommending that cross-sectional imaging be used for assessment of all dental implant sites. Cone-beam Computed Tomography (CBCT) is the cross-sectional imaging method of choice. The cross sectional view provides critical information that cannot be gained from any purely 2D modality. The example below shows the cross sectional view.

What is the Field of View (FOV)?
The Field of View (many times referred to as FOV) refers to the size of the volume captured in the scan. Almost all CBCT systems on the market capture a volume that is shaped like a cylinder (i.e. a tin can). Therefore, the FOV is expressed with two numbers, which are typically in cm. The first number typically refers to the diameter of the circular face of the cylinder (the width of the tin can). The second number refers to the height.

The FOV typically advertised by a dental cone beam system will represent the largest FOV that can be captured by the system. However, almost all systems will offer the flexibility to perform smaller scans as well (in other words, a system that advertises a 16 x 8 FOV will also typically offer the option of scanning smaller volumes like 8 x 8, 8 x 10, or 4 x 6, etc. However, a system listing as a 8 x 8 FOV typically means that a larger scan is not an option with that system.
How big of an FOV do I need?
While there are many different options on the market, we sometimes put the different FOV sizes into three main groups.
First are the very large FOV machines are those that can capture most of the cranium in a single scan (e.g. largest scan size of 16 x 16 and above). These systems will be the most expensive and are typically used by oral surgeons or other specialists.
Second are the smaller FOV machines (e.g. 8 x 8 or 10 x 10). These can be an adequate dental cone beam system, as it allows capture of most of the essential anatomy. Below is a sample of a volume in this range (3D reconstruction, axial and sagittal views):

Potential challenges with cone beam systems that max out at this size may include:
- Cutting off 3rd molars
- Inability to perform airway analysis
- Inability to capture both TMJs in a single scan
- Little margin for error in patient positioning (i.e. suboptimal positioning may cause desired anatomy to fall outside the scanning volume)
Third are the medium size FOV dental cone beam machines (e.g. 16 x 8). Below are examples of a 16 x 8 volume (3D reconstruction, axial and sagittal views):

What about 2D panoramic radiographs?
Most dental cone beam systems today can also create 2D panoramic radiographs. However, what many dentists aren’t aware of is that the panoramic capability of dental cone beams can vary dramatically. This stems from the fact that dental cone beams typically generate their panoramic in one of two ways.
The first type of dental cone beam will utilize the 3D sensor to create the panoramic radiograph. This approach will allow the manufacturer to save money. However, the trade-off is that the panoramic radiograph will typically suffer in image quality, because a flat panel 3D sensor is not optimized for a 2D scan.
The second type of dental cone beam possesses a separate sensor that is dedicated to and optimized for panoramic radiographs. One example is a cone beam that has a Direct Conversion panoramic sensor, which is designed to reduce noise in panoramic and cephalometric scans.
It’s worth noting that you would never know which type of cone beam you have by looking at it, because this is all happening “under the covers” (so to speak). The noticeable difference will be in the panoramic scans.
What is the difference in patient dosage with a dental cone beam as compared to other modalities?
To answer this question, it’s worth a quick definition of how dosage is typically quantified. The most common approach to describing x-ray dosage is called “effective dosage”. Effective dosage takes into account the anatomy being exposed in additional to the power of the exposure to provide a more accurate indication of health risk. The typical unit of measurement is the “sievert” (Sv), or more commonly in the dental realm, the “microsievert” (μSv).
Dosage for a cone beam scan is going to vary based on the parameters of the scan (FOV, kVp, mA, and exposure time, etc). However, one study performed a few years ago (1) measured a number of medium sized FOV cone beams and found the effective dose to range from 83 μSv to 194 μSv.
A typical panoramic x-ray can result in an effective dose of about 14 μSv. A typical full mouth series (FMX) that includes 18 intraoral radiographs results in about 171 μSv of effective dose (2).
Finally, to help patients put the dosage numbers into perspective, it may be worth comparing these to some common phenomenon from everyday life. According to the United Nations Scientific Committee on the Effects of Atomic Radiation, the average worldwide background radiation is about 2400 μSv per year or approximately 7 μSv per day. A cross-country flight is about 30 μSv. A medical chest CT is 7000 μSv. While some patients can understandably get concerned about “CT” scans, it’s worth noting that dental CBCTs are a fraction of the dose when compared to medical CT scans.
Will a dental cone beam system integrate with my existing systems?
Integration is always a concern because almost every dental digital system is dependent on other parts of the workflow to deliver the quality patient care. To organize ourselves, we will break it into two categories: 2D images (pans and cephs) and 3D volumes.
For 2D panoramic x-rays and cephalometric images, integration is typically very straightforward, as the 2D images will be automatically exported into the office imaging software (i.e. the same software used to manage the intraoral images). This interface may be a proprietary direct interface, or could be utilizing the industry-standard called “TWAIN”. Either way, it’s no different than how a traditional panoramic x-ray would interface with the imaging software for an office.
For the 3D volumes, typically the cone beam system will come with its own dedicated 3D management software. This software will typically allow a given 3D scan to be shared throughout the office.
There are scenarios where the office will need to use this 3D data for other purposes, like working with a lab, 3D printing surgical guides or milling crowns. To determine if the 3D volumes integrate with the various other systems involved in these applications, there are two primary file formats that play a big role.
The first file format to be aware of is DICOM, which is a standard format for digital medical images. Most dental cone beam volumes are made up of hundreds of 2D DICOM files (these are the “slices” that are created by the CBCT when a scan is performed).
Most dental cone beam systems create 3D volumes that are DICOM format. This is important for things like opening volumes in other 3D software (if an office has a preference for 3D software that is different than that provided by the cone beam manufacturer). DICOM format will also be important if the volume is provided to a lab who will then create the actual implant or will 3D print a surgical guide. Typically, the lab will have specialized software that allows them to merge your DICOM format volume with data from an impression (whether this impression was generated via a physical model or optical scanner).
The second file format to be aware of is called STL (short for stereolithography), which is the industry standard for 3D printers and CAD/CAM (Computer Aided Design/Manufacturing). This format becomes important when 3D printing or milling is done.
Some cone beam systems also offer the option of outputting the volume (or parts of the volume) in STL format. This capability becomes important if an office plans to be more involved in the creation of implants, surgical guides or other appliances in-office. If this capability is important to an office, it is worth checking whether the cone beam software can output STL formatted volumes. Furthermore, it is also worth asking whether STL output comes standard with the Cone Beam software, or if it’s an add-on surcharge.
Is there an increased legal liability with a CBCT?
As you might expect, any time we wade into this area, our own lawyers request we remind everyone that we are not legal counsel, and you should always refer to legal professionals. However, we are happy to share a few thoughts.
To lose a lawsuit, typically a patient must prove that injury due to negligence was avoidable. When it comes to placing implants, most legal advisors seem to recommend that there is much greater risk in NOT taking a CBCT scan. This is because if there are complications and a CBCT was not taken, a court could determine that injury could have been avoided had the doctor gained additional information that a traditional dental cone beam scan could have provided.
Regarding liability with reading a CBCT scan, the general consensus is that at a minimum, any provider who acquires CBCT scans is liable for not recognizing abnormalities or pathologies on any cuts used for the clinical indication.
Some dental practices attempt to protect themselves by having patients sign a waiver. The opinion that seems be shared amongst the legal community is that waivers of liability have no legal effect and courts will ignore them. Most jurisdictions that have considered the matter have held that physicians and hospitals cannot require patients to waive their rights to recover damages for negligence.
Given that reading CT scans is a specialty in its own right, there is also consensus that more training is always a positive thing for the dental professionals who are acquiring 3D scans for the first time. There are myriad courses both online and in person offering additional training on this topic. Seeking out that training has no downside.
What determines image quality?
There are a host of different factors that can affect the resulting image quality ranging from positioning to the mode selected (modes that utilize longer scans and smaller volumes would have high resolution). However, we thought it would be worthwhile to highlight a few key factors that can vary by equipment manufacturer.
The focal spot size of any x-ray modality defines the edge definition of the object being imaged. This is true whether it be a wall mounted x-ray, panoramic x-ray or dental cone beam. The smaller the focal spot, the higher the precision of the radiographs. This focal spot size can vary dramatically in panoramic and cone beam systems with some focal spots as large as 0.7 mm and some as small as 0.2 mm.
The voxel size for 3D volumes represents the precision of the spatial resolution of the 3D volume. The smaller the voxel, the higher the resolution. It’s also important to note that the voxel size will also vary depending on the field of view that is used in a given scan. Therefore, because (as mentioned above), most dental cone beam machines offer options for the Field of View (i.e. different size scans can be performed on the same unit) – that means that the voxel size will vary across different FOV sizes on the same cone beam machine. The larger the Field of View, the larger the voxel size and the lower the resolution. The voxel size of most systems will typically vary anywhere between 70 micrometers to 400 micrometers.
For many (if not most) offices that use a dental cone beam, the panoramic x-ray modality is used more frequently than the 3D modality. Given this, it’s important to note that not all dental cone beams create their panoramic x-ray radiographs the same way. These typically fall into three categories:
The first type uses the same sensor to perform both the 3D scan as well as the 2D scan. With these systems, they are typically optimized for the 3D scans while the 2D panoramic scans can be suboptimal, which can lead to lower quality panoramic x-rays. For instance, a typical high-quality panoramic x-ray would have a pixel size of 100 micrometers…. However, a 3D flat panel sensor with that level of resolution would typically be too expensive, so the design typically makes do with a lower resolution panoramic image. These units may be ideal for offices for which the 3D scans are a much higher priority (and higher frequency) than the panoramic x-rays.
The second type uses a dedicated sensor for panoramic x-rays. However, the material used in the 2D sensor does not have the ability to convert the x-ray directly to a digital signal. These sensors must convert the x-ray to light first, then convert the light to a digital signal. This double conversion can result in a loss of image resolution in the resulting digital radiograph.
The third type also uses a dedicated sensor for panoramic x-rays, but they utilize a Direct Conversion Sensor. This means that the material used in the sensor is sensitive enough to x-ray radiation to be able to convert the signal directly to a digital signal, which allows the signal to retain its precision in the resulting digital radiograph.
Are there special requirements to install and operate a dental cone beam in my office (different from other dental x-ray equipment)?
The requirements for dental cone beam installation and operation typically are defined at the state level. However, larger cities (e.g. New York City) may have additional unique requirements. While the company you purchase the unit from should be able to advise you on your local requirements, there are a few main areas to be aware of. The last thing anyone wants is an inspector telling the office that they are out of compliance after everything is installed.
First involves the certification of the installer and the operator. Most states require that the installer be registered with the state as a certified x-ray technician. Sometimes, states will also ask that operators be registered as well.
Second involves the certification of the office layout. Some states have requirements to submit an office plan to the state for review and approval. Some states require evidence that a radiation physicist has reviewed the plan.
Third involves ongoing maintenance and quality assurance. Most states ask that the office simply follow the recommendations of the manufacturer (which are typically outlined in their manual). However, some states may have additional requirements.
All of these items are typically not difficult to perform and follow. However, it is important to be aware of them.
Dental Cone Beam System is a big investment for any office. Understanding the pros and cons of different designs will help your team make sure there are no surprises. If you have any questions, please give us a call to talk to one of our specialists.
Learn more about ImageWorks Cone Beam Solutions
1 – “Effective dose range for dental cone beam computed tomography scanners”, European Journal of Radiology; Aug, 2010
2 – “Patient risk related to common dental radiographic examinations: the impact of 2007 International Commission on Radiological Protection recommendations regarding dose calculation” published in The Journal of the American Dental Association in 2008
Subscribe to Receive More Great Articles