 One of the biggest challenges that dental offices face with digital sensors is knowing whether things will work together. It seems like it should be so simple to just add or replace a sensor. However, for so many offices in this situation, they will hear high-priced imaging systems claim “nothing else will work”, while low-priced systems may claim “it will work with everything”.
One of the biggest challenges that dental offices face with digital sensors is knowing whether things will work together. It seems like it should be so simple to just add or replace a sensor. However, for so many offices in this situation, they will hear high-priced imaging systems claim “nothing else will work”, while low-priced systems may claim “it will work with everything”.
The reality is usually somewhere in the middle depending not only on what systems are currently being used, but also what your needs and expectations are. More and more, we are hearing from dental professionals who want to understand the tradeoffs more clearly. The reason is that with a little knowledge, the office can save quite a bit of money without sacrificing image quality or workflow efficiency.
With this goal in mind, we wanted to shed some light on some of the most common questions we hear from dental professionals when they are looking to implement a new dental digital intraoral sensor system.
1. Does the intraoral dental sensor need to be compatible with my x-ray unit? Typically, you do not need to worry about compatibility between your intraoral dental sensor and your intraoral x-ray unit as most sensors will work with most x-ray units. While the optimal settings on that intraoral x-ray unit may vary somewhat for that particular sensor (e.g. using handheld x-rays), this is easily adjustable. Therefore, a sensor will work with almost any intraoral x-ray unit.
2. What’s the difference between a size 0, size 1, size 1.5, and a size 2 sensor? A size 2 sensor is typically referred to as an “adult” size sensor. Typically, manufacturers who offer a size 2 sensor also offer a size 1, or a “pedo” sensor. Alternatively, some manufacturers offer a single 1.5 size which is meant to be a size in between a size 1 and a size 2. The tradeoff with any size sensor is patient comfort vs. size of the field of view. A larger sensor will have a larger field of view (and therefore, more diagnostic value). However, a larger sensor also tends to be less comfortable for the patient. Some offices may prefer the size 1.5 as a “one size fits all”, while other offices may prefer the larger FOV that a size 2 brings for adults, while also having a size 1 that a child will be able to fit in their mouth.
The size 0 sensor is a very small sensor often times offered as an even smaller pedo sensor. Here’s a fun fact about the size zero sensor: the origin of this sized sensor stems from manufacturers looking for ways to better utilize the excess sensor material that would otherwise have been scrapped (because cutting rectangular sensors from a round “wafer” results in leftover material). There was little incremental cost to make this excess material into an even smaller sensor (because the material would have been scrapped anyway). This tiny sensor was labelled a “size 0”, and it has a very small field of view.
3. Can I move my sensors between rooms? Absolutely. Most modern sensors have simple connections to the USB port of a PC.
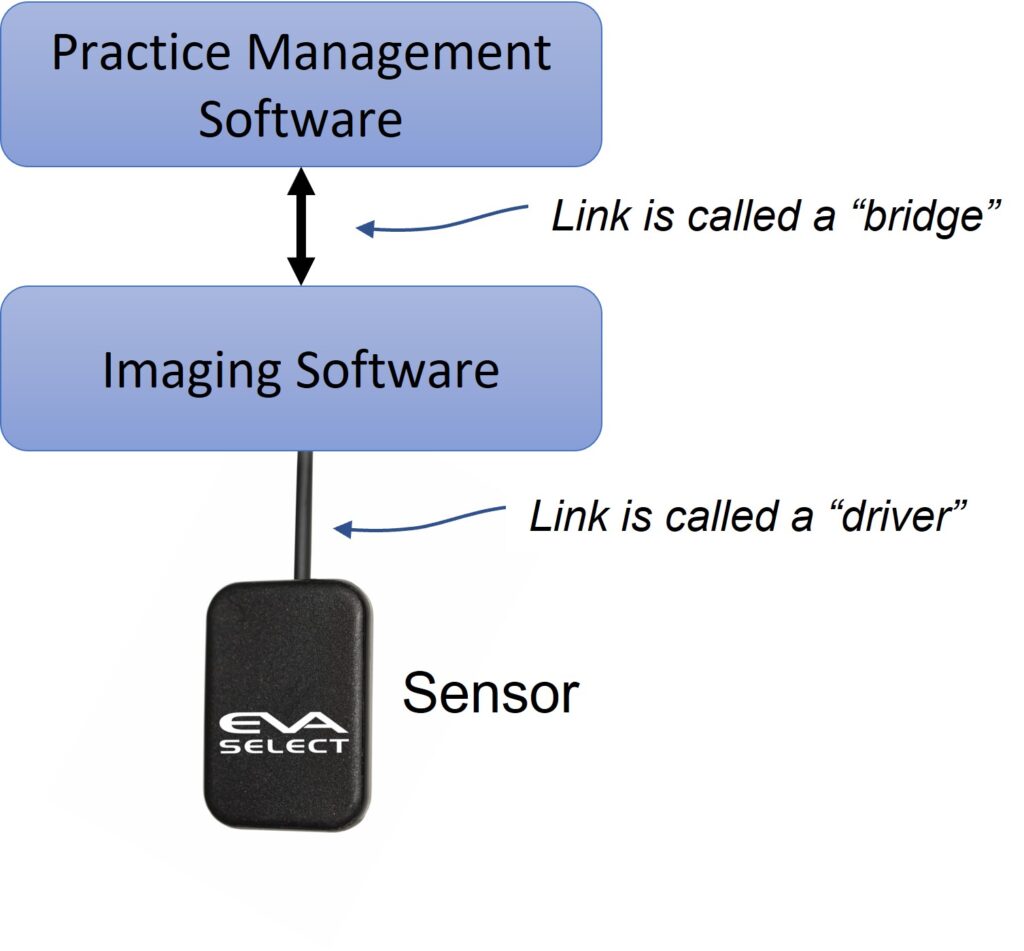
4. Is it easy to change sensor systems? Frequently, the answer to this question depends both on the system you are using and what’s important to you. It’s first worth a quick explanation of the relationship between the sensor, the imaging software, and the practice management software.
In most digital systems, the sensor is controlled by the imaging software, so the ability of the system to work is dependent on the ability of the imaging software to control that sensor. Many times, people simply think of the sensor as an independent piece of hardware, like the tire of a car that can be easily changed. While this is becoming more common, it’s more accurate to think of the sensor and the imaging software as one system. Therefore, answering this question is usually dependent on the ability of your imaging software to accept other sensors, as well as the ability of your sensor to work with your imaging software. Some more detail of typical scenarios are explained below.
It’s also worth noting that sometimes the imaging software may actually be provided by the practice management software provider. In these cases, it can be confusing because it may not seem like there is a separate software for the imaging.
5. Can I use any sensor with my current imaging software? As mentioned above, the answer to this question depends not only on the system you are using, but also on what’s important to you. Typically, plugging a sensor into a PC that uses another imaging software results in one of three common scenarios:
Scenario One: the imaging software cannot accept the image captured by the sensor. The sensor will not work with the software.
Scenario Two: the imaging software can capture the image, but the software will not offer any “capture automation” capabilities for that sensor. For example, during a multi-image study, the user may have to click to accept each image in the software before moving to the next position. Sometimes, the user may also have to manually rotate and place the images in the correct charting position.
Scenario Three: the software can capture an image and apply the same automation capabilities that its own sensor would have.
Some offices may see Scenario Two as unacceptable, while other offices may be ok with this if they are saving money. To further complicate matters, sometimes either the imaging software or the sensor (or both) may have the potential to work together to achieve Scenario Two or Three above, but they may require additional pieces of software to do so. In most cases, this additional software comes from the sensor provider, and is called a “driver”. A “driver” is a generic term for a small piece of software that is provided by the hardware manufacturer to “handshake” with a larger software application (e.g. a “TWAIN” driver is a very common one). It’s also worth noting that at least one large software provider charges fees simply to allow someone else’s sensor driver to work with their software.
6. I would like to (or need to) change my imaging software. Does my imaging software need to work with my practice management software? The communication between the imaging software and the practice management software is typically referred to as a “bridge” (see image above). First, it’s worth mentioning that the imaging software can operate independently from the practice management system (i.e. without a bridge). However, if they do work together, there are some workflow advantages to this. Typically, the bridge offers two things:
1. The ability to open the imaging software directly from the Practice Management software, so that less clicks are required, and the patient being imaged will be automatically selected in the imaging software (i.e. no need to search for patient again in the imaging software after the patient was already looked up in the practice management system).
2. For new patients, the patient information that is entered into the Practice Management system is automatically updated into the imaging software thereby avoiding redundant data entry for new patients.
In general, the bridge will make the user feel like the practice management software and imaging software are one piece of software.
7. If I change my imaging software, what should I do with all the images that are stored in my current software? Typically, the imaging software is what stores and manages all your digital x-ray images. If you change your imaging software, new images will be stored and managed in the new imaging software. Assuming the new software is not able to simply connect directly with the existing database of images, typically, you have two main options for what to do with the images in your old software.
Option one, is to simply keep a copy of the older software that you already have and use it to access the older images. These images would also typically be archived and backed up as part of the normal IT best practices. With this approach, there is usually a short period where comparing images taken at different times for a patient would require either printing, or exporting certain studies. However, after a short period, the need to refer to older images becomes less and less frequent.
Option two applies if both the old software platform and the new software platform are compatible. If they are, the images may be able to be “ported” to the new software so that the old images would be available in the same place as the new images. Typically, if porting is possible between the two software platforms, it would be a separate service that would be offered by the software company for an additional charge.
The digital intraoral dental sensor is a critical component for a busy dental practice. Understanding some of key components involved in implementing a new sensor in your office will help your team make the most of their investment as well as make sure there are no surprises.
If you have any questions, or would like to better understand the tradeoffs of different options, please reach out to talk to one of our specialists.
Subscribe to Receive More Great Articles