Subscribe to Receive More Great Articles
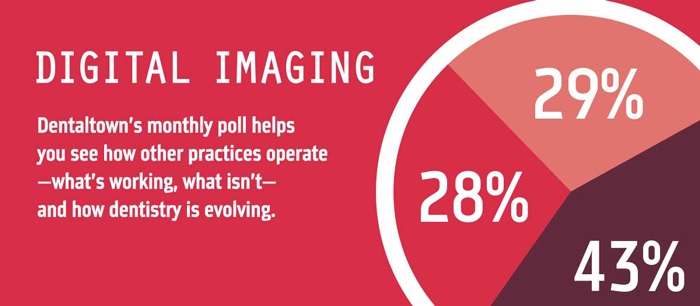
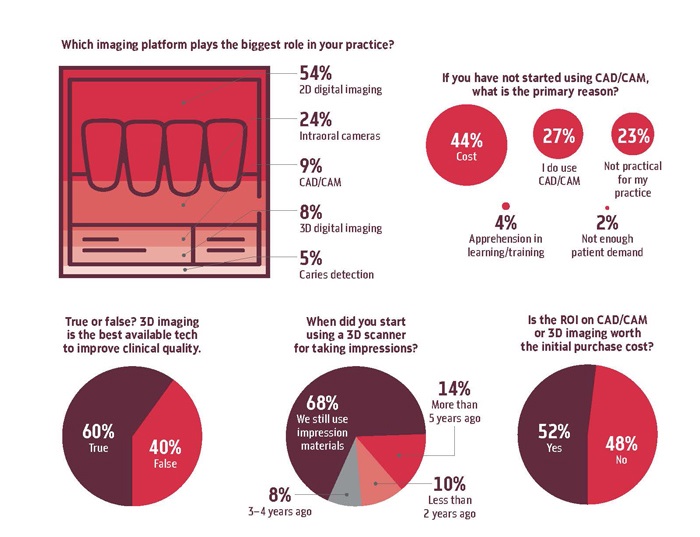
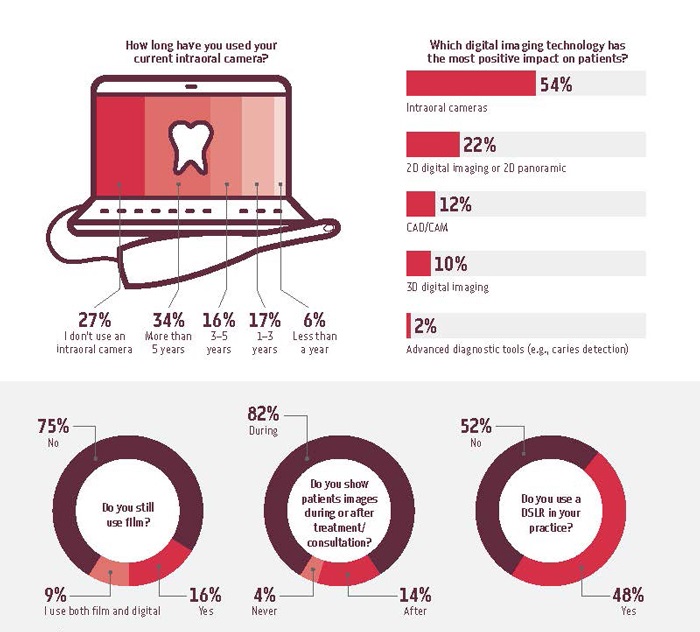
Dentaltown Survey on Dental Imaging
Dentaltown has recently released a new poll summarizing trends in digital imaging.
Learn more about ImageWorks Solutions
Panoramic and Cephalometric Systems
One Simple Thing To Alleviate Patient (and Parent) Fear of Cone Beam Scans
 One the biggest challenges that dental professionals have is reducing patient anxiety and fear. In fact, increasing comfort and reducing anxiety is a main driver in patient retention for a successful dental practice. One area of opportunity comes with the cone beam scan in a dental office.
One the biggest challenges that dental professionals have is reducing patient anxiety and fear. In fact, increasing comfort and reducing anxiety is a main driver in patient retention for a successful dental practice. One area of opportunity comes with the cone beam scan in a dental office.
If you feel that the cone beam scan is appropriate, the patient may already be on edge. Perhaps the patient has never had a cone beam scan before, and doesn’t know what to expect. Many times, the patient (or the patient’s parent) will feel their anxiety spike higher with concerns of radiation risk. In fact, many patients may, consciously or subconsciously, use the logic that “wow, they are bringing out the big guns – this must be serious!”
Sometimes, counteracting this anxiety can be as simple as the words that are used. Our recommendation: don’t call it a “CT”.
Of course, it’s correct to call it a CT, as this stands for Computed Tomography, and is the general umbrella of all modalities that use this technique to gather data in three dimensions. It includes MRI and Catscan systems used in hospitals, as well as the dental cone beam.
The full abbreviation of CBCT, stands for Cone Beam Computed Tomography, and while it uses similar technology as these larger systems used in hospitals, the “Cone Beam” portion of the name highlights the key difference that will make your patient feel much better: the radiation dosage from a dental cone beam is a tiny fraction of that from a traditional CT they would find in a hospital.
However, when you use the phrase “CT” or “Dental CT”, the patient may associate the scan he or she is about to get with these larger machines. They may also associate these machines with larger radiation output, higher risk, and more serious diagnoses.
Given these associations, we believe it is more comforting to the patient to call it a “3D scan”, “cone beam scan”, or simply a “scan”. Using these words may alleviate the patient from additional anxiety.
What is DICOM vs. STL in 3D Dentistry?
As more and more of the world of dentistry moves into 3D, there is a collision of two different data standards: DICOM and STL. To understand these standards and the roles that they play, it may be helpful to understand where they come from.
The first data format is called DICOM, which stands for Digital Imaging and Communications in Medicine. For decades, this has been the standard for all medical digital radiography. It not only covers the formats to be used for storage of digital medical images, but also covers the protocols related to the communication services which are useful in the medical imaging workflow. Now, in the dental arena, digital radiographs are typically DICOM standard mainly to drive consistency in image file format. The protocol standards that are defined by DICOM are less relevant to a typical dental office because they are used when communicating with a Picture Archiving and Communication System (PACS). PACS are used in larger facilities (e.g. hospitals, prisons) that have a wide variety of digital radiographs that need to be performed, stored and managed.
In a dental office, the traditional cone beam scan are typically stored by the imaging software in DICOM format. For a dental cone beam, the data that makes up the volumes actually consist of many (typically hundreds) of 2D slices. Each of these slices is also typically in DICOM format.
The second data format that has become more important to dentistry recently is STL, which is short for stereolithography (You might also hear it referred to as Standard Triangle Language or Standard Tessellation Language). This format has it’s origins in the fields of 3D printing and Computer Aided Design and Computer Aided Manufacturing (sometimes referred to as CAD/CAM). It describes the surface geometry of a three-dimensional object and has become the data format that most 3D printers and milling systems require. In a dental office, the traditional intraoral scanner will output in STL format.
While the DICOM approach to 3D breaks the volume into slices. The STL format breaks the surface of the volume down into “tiles” which are typically triangular. As a result, the DICOM file tends to provide more information about what’s inside the volume, while the STL file tends to provide more information about the surface of the volume.
When creating an implant plan, clearly both of these types of information become very useful. Particularly when a surgical guide is being created because it utilizes information underneath the surface but also needs to know information about the surface itself including the soft tissue.
Commonly, the dental office does not need to worry about converting one format to the other because this is generally where the lab plays a role. The lab has deep expertise and software tools to help them merge these different formats together to create the implant plan for the dental professional. However, if a dental office would like to start performing chairside milling, or printing their own surgical guides, then it becomes more important to understand how these data formats work together.
How Big of a Field of View Do I Need for My Dental Cone Beam?
At ImageWorks, we’ve been helping dental practices make the most of their dental imaging for decades. When it comes to dental cone beam systems, technology has come quite a way since we introduced our first generation 3D dental cone beam system in 2005 when we were called Dent-x.
As technology advances, we are always excited to introduce a dental professional to the power and value of 3D imaging, because it is compelling for so many offices. However, at the same time, with today’s 3D cone beam systems, we also like to say: with great power comes great responsibility. Because of this responsibility, we think it’s important to offer information that allows new users to enter the world of 3D with eyes wide open.
With this goal in mind, we thought it would be worthwhile to provide an overview of some of the most common questions that get asked when dental professionals are looking to implement a Cone Beam system in their office. We hope you find this useful.
What is the Field of View (FOV)?
The Field of View (many times referred to as FOV) refers to the size of the volume captured in the scan. Almost all CBCT systems on the market capture a volume that is shaped like a cylinder (i.e. a tin can). Therefore, the FOV is expressed with two numbers, which are typically in cm. The first number typically refers to the diameter of the circular face of the cylinder (the width of the tin can). The second number refers to the height.

The FOV typically advertised by a dental cone beam system will represent the largest FOV that can be captured by the system. However, almost all systems will offer the flexibility to perform smaller scans as well (in other words, a system that advertises a 16 x 8 FOV will also typically offer the option of scanning smaller volumes like 8 x 8, 8 x 10, or 4 x 6, etc. However, a system listing as a 8 x 8 FOV typically means that a larger scan is not an option with that system.
How big of an FOV do I need?
While there are many different options on the market, we sometimes put the different FOV sizes into three main groups.
First are the very large FOV machines are those that can capture most of the cranium in a single scan (e.g. largest scan size of 16 x 16 and above). These systems will be the most expensive and are typically used by oral surgeons or other specialists.
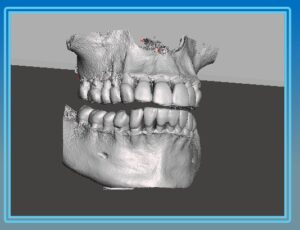
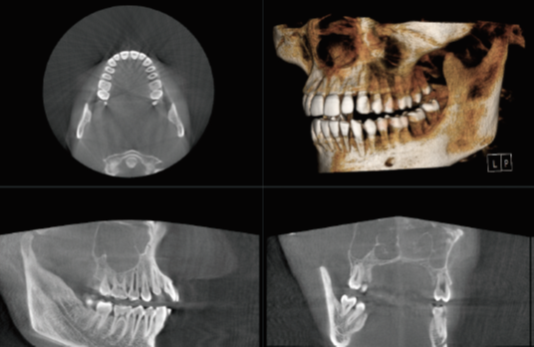
Second are the smaller FOV machines (e.g. 8 x 8 or 10 x 10). These can be an adequate dental cone beam system, as it allows capture of most of the essential anatomy. Below is a sample of a volume in this range (3D reconstruction, axial and sagittal views):

Potential challenges with cone beam systems that max out at this size may include:
- Cutting off 3rd molars
- Inability to perform airway analysis
- Inability to capture both TMJs in a single scan
- Little margin for error in patient positioning (i.e. suboptimal positioning may cause desired anatomy to fall outside the scanning volume)
Third are the medium size FOV dental cone beam machines (e.g. 16 x 8). Below are examples of a 16 x 8 volume (3D reconstruction, axial and sagittal views):

For most cone beam systems, the field of view represents the largest volume that can be captured. In other words, the user has the option to scan smaller volumes, but not larger.
In the end, the decision is a matter of what limitations the dental professional can tolerate versus the cost. Typically, the larger the field of view, the higher the price. However, at the same time, the larger field of view provides less limitations on what the user can capture.
Subscribe to Receive More Great Articles
How does radiation exposure compare between common dental x-ray modalities?
A common challenge we have heard from many dental professionals is how to weigh the tradeoffs that come with these advanced capabilities vs. the increased radiation exposure that comes with them. While the principles of ALARA (As Low As Reasonably Achievable) are of the highest concern, practicing it requires an understanding of the basics of radiation.
To help patients put the dosage numbers into perspective, it may be worth comparing these to some effective doses of common phenomenon from everyday life. According to the United Nations Scientific Committee on the Effects of Atomic Radiation, the average worldwide background radiation is about 2400μSv per year or approximately 6.7 μSv a day. A cross-country flight is about 30 μSv. Using these estimates, we can do a rough comparison with every day experiences (CBCT values are the median of the ranges above).
| Study | Effective Dose (μSv) | Days of Background Radiation | Cross Country Flights |
| FMX (round cone) | ~150 | ~22 | ~5 |
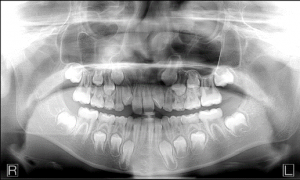
| Panoramic X-ray | ~10-15 | 1-2 | < 1 |
| Small FOV CBCT | ~30-100 | 4-15 | 1 – 3 |
| Large FOV CBCT | ~100-500 | 15-75 | 3 – 16 |
Subscribe to Receive More Great Articles
Dr. Smith and Dr. Johnson: Two Approaches to 3D Dentistry
Dr Smith and Dr. Johnson: Two Approaches to 3D Dentistry
Over the years, ImageWorks has helped thousands of offices make the most of their digital imaging. We wanted to share a thought about two common scenarios that we often see with dental professionals utilizing cone beam technology in their practices.  Let’s describe these in terms of two practice owners. We’ll call them Dr. Smith and Dr. Johnson.
Let’s describe these in terms of two practice owners. We’ll call them Dr. Smith and Dr. Johnson.
When it comes to evaluating a Cone Beam, Dr. Smith sees this simply as a cost that needs to be endured, and he thinks of the ROI simply in terms of how much he can get paid for every scan. Therefore, Dr. Smith’s number one objective is simply to minimize that cost as much as possible. With this objective, Dr. Smith will be able to find a cone beam that will be dropped in their office, and Dr. Smith will be on his own. Three months later, the doctor finds that the staff is a little afraid of taking a 3D scan because they have not done many. Perhaps early on, some staff members who only received an hour of training when the unit was installed, didn’t have their first cone beam patient until 3 weeks later. At this point, perhaps they forgot the positioning technique and ended up cutting some anatomy off in the scan. After this experience, the staff became afraid to use it. One year later, the office is only using the system for panoramic scans, and because the unit was designed to use one sensor for both panos and cone beams, in the end, the office has paid a lot of money for a low-resolution panoramic x-ray.
Dr. Johnson, on the other hand, sees the cone beam system as an investment. She knows this investment has the opportunity to enhance her practice in a number of ways:
- Her staff will be able to create longer-term consulting relationships with her patients from day one. This will allow the practice to have more engaged, longer term discussions with patients, which will make the patient base of the practice more consistent, and the billing more stable.
- Her staff will spend less time convincing patients of the accuracy of the diagnosis because the patients will be able to see for themselves. More time can be spent discussing treatment options and actually performing dentistry.
- She will have more confidence in speaking with patients about the treatment plan options, because she has so much more information to determine probabilities and risks.
- If she does come across pathology that she is not familiar with, she can easily provide plenty of information to a specialist. If that specialist does not know, she can easily engage with a maxillofacial radiologist. She knows that each one of these situations creates further opportunity for learning, because every time she engages a specialist review, she will now be familiar with this pathology next time around. Over time, all this additional information across all of her patients accelerates her knowledge and experience, and there is an exponential growth in learning.
If you have questions about whether a cone beam system could improve you practice, sign up for a 15-minute introduction with us. We would love to chat with you.
How Far Has the Dental Industry Rebounded?
As bleak as things looked in April for dental practices, May showed signs of life and indicators of a potential quick recovery. However, at that time, uncertainty still prevailed. Now, as the ADA survey results for the first week of June are in, the rebound continues on it’s robust trajectory.

The ADA released their latest data in which they survey members on a number of questions related to their current activity. For the week of June 1st, they found another dramatic increase in dental practice volume. This was marked both by the percentage of practices saying they saw an increase in patient volume…

…as well as the percentage of practices saying they began seeing non-emergency patients. Furthermore, almost 20% of dentists in the survey responded that patient volumes are at or close to normal levels again.
As expected, these levels are not consistent everywhere as certain states are slower to open. For instance, in New York about 59% of dentist say they are still at less than 25% volume. Pennsylvania is at similar levels. Meanwhile, only about 12% of dentists in Florida were still operating at less than a quarter of typical patient volumes.
Overall, a great trend that we will continue to keep a close eye on.
Subscribe to Receive More Great Articles
Test Post
Test post

The Number One Challenge When Adding a Dental Panoramic X-Ray to a Hospital or Urgent Care Clinic
Background
There is a growing desire by health care facilities to add panoramic dental x-ray modalities to their capabilities. The main reasons for this are a combination of the panoramic x-ray’s broad diagnostic capabilities along with it’s low cost and low radiation relative to other traditional medical imaging modalities. Here are three common applications:
1. Emergency rooms and urgent care facilities value the targeted anatomy and field of view as be an ideal modality to assess facial trauma. For example, as more of these facilities are seeing patients with severe or emergency dental ailments, the staff values the panoramic dental modalities to help determine whether the patient should be referred to a dentist or to another specialist.
2. Surgical centers used by dental surgeons that utilize the panoramic image to capture pre and post-surgery x-rays.
3. Self-contained facilities, like military bases, prisons and native american reservations, that must provide full health care to a specific population. In these scenarios, the facility values the multi-purpose modality that not only can provide dental care, but also offer the broader capabilities mentioned above.
Challenges
One of the main challenges that these facilities face is integrating these pieces of equipment with their facility PACs. The main driver behind this challenge is that most of the panoramic x-ray solution providers are more familiar with traditional dental offices and dental office workflows. Therefore, most panoramic x-rays are designed and optimized to work in this environment. Unfortunately, Imaging Centers, Health Clinics and Hospitals use very different information systems and workflow, whether it be how procedures are ordered, or how the image is scanned, reviewed and diagnosis performed. Typically, the central hub for x-ray images in these facilities is the DICOM protocol PACs system.
What is PACs?
PACs is an acronym for Picture Archiving and Communication system. This is a unified network of systems that allow many types of medical imaging data available for modern medical diagnosis (e.g. MR, CT, Ultra Sound, etc) to be effectively and efficiently collected, stored and viewed between the various practitioners involved in the care and treatment of a patient.

In a typical workflow, a primary or emergency physician will first order a particular image study. Then the patient will go to the radiology department where a radiology technician will perform the imaging procedure. The images will then be routed to a Radiologist who will perform a reading and create a report. This report may contain imaging data diagnosis and treatment recommendations, which would then be sent to the referring physician. The PACs is the part of the hospital information system (HIS) computer network that supports this activity.
What is DICOM?
DICOM is an acronym for Digital Imaging and Communications in Medicine. This is the standard protocol that PACs systems and PACs connected equipment use to work as a system. The set of DICOM standards are the common rules specifically created and targeted to storing and sending medical diagnostic imaging data that allow independently designed software and hardware to interconnect with each other. This is analogous to the internet where MACs and PCs use Chrome, Firefox or Safari browsers to access websites running on someone else’s servers. They accomplish this by implementing various web standards such as https and www.
Who controls DICOM and why was it created?
The DICOM standards are controlled by the DICOM Committee of NEMA (National Electronic Manufacturers Association), an industrial trade organization. The impetus for the creation of DICOM standards was to make cross-vendor PACs a reality. It enables the CT, MR, CR and other diagnostic image sources from different manufacturers to integrate with image archiving and display systems. Furthermore, DICOM-compliant systems can be configured to work together no matter who manufactured the equipment or developed the software.
Are there different versions of DICOM?
The current version of DICOM is Version 3.0. However, that is only part of the answer. The complete DICOM standard is very broad to cover just about anything you can find in a hospital or imaging center that is related to diagnostic imaging. The DICOM standards are regularly updated and extended to cover changing equipment (called “modalities” in DICOM-speak) and the requirements of the various specialties that comprise modern medicine.
Can DICOM image files be viewed on any computer?
Usually software created to open DICOM images are needed to view DICOM images. This is because DICOM images usually contain additional information, called “metadata” about the patient, the image capture and display instructions. This metadata is typically not visible when viewing the images on a screen.
Can a digital Dental Panoramic X-ray Scanner be installed in a PACs?
Yes, if the panoramic system is DICOM compliant.
How do I connect to the PACs?
You will typically connect to the hospital LAN with a standard ethernet cable and will need to configure settings to make connections to 2 distinct systems within the hospital PAC system:
1. A connection to the Modality Worklist Server: This is the system where the operator pulls the list of patients scheduled for procedures. This allows the details of the patient and study (such as patient name, ID, age, sex, etc.) to be automatically input to the dental panoramic system.
2. A connection to the Image Storage Server: This is the system that files and stores the images generated by the digital panoramic system so that they can be retrieved and viewed by the radiologists, referring physicians and other medical staff that have access to the system.
What information do I need to give the Hospital’s PACs administrators to connect a DICOM Compliant Panoramic X-ray to an existing PACs system?
You will need to speak with the PACs / DICOM department and will need to give them the following information about the Dental Panoramic X-ray.
- The units IP address
- The units AET or AE Title (Application entity title)
- The DICOM modality for the equipment.
What information do I need to get from the Hospital’s PACs administrators to connect a DICOM Compliant Panoramic X-ray to an existing PACs system?
You will need to speak with the PACs / DICOM department and will need to get the following information regarding the PACs.
For the Modality Worklist Server
- The Modality Worklist Server’s IP address
- The Modality Worklist Server’s Port
- The Modality Worklist Server’s AET or AE Title (Application entity title)
For the Image Storage Server
- The Image Storage Server’s IP address
- The Image Storage Server’s Port
- The Image Storage Server’s AET or AE Title (Application entity title)
What staff training will the department expect and require?
Typically, the radiological technicians on staff will be much more familiar and comfortable with computerized image system but have less experience with panoramic X-rays than staff in a general dental office. It’s important to make sure the trainer understands the unique workflow of the particular facility.
Learn more about panoramic x-rays
Learn more about cone beam systems
If you have questions about how a hospital, urgent care facility or surgical center might benefit from a Panoramic X-Ray, reach out to us, and we would happy to answer any questions you have.
Subscribe to Receive More Great Articles